Language can be broadly separated into speaking (producing spoken language), understanding (comprehending spoken language), writing (producing written language) and reading (understanding spoken language). None, some, or all of these areas may be affected following stroke or other neurological damage. This may mean, for instance, that a person is able to read but not write, to talk but not understand, to sing but not talk. Our body ‘language’ including gesture and facial expression, as well as subtle changes in our prosody when we speak also affects the meaning of the message we are trying to convey or understand.
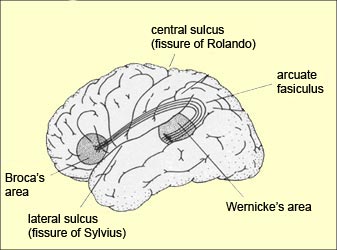
Picture from here http://thebrain.mcgill.ca/flash/d/d_10/d_10_cr/d_10_cr_lan/d_10_cr_lan.html
When a person presents with an acquired language impairment following neurological damage we call this Aphasia. This is usually caused by damage within Broca's area, Wernicke's area or the 'language loop' connecting to the two within the person's left hemisphere. The severity of aphasia may lie anywhere on a spectrum from very mild to very severe. Aphasia can impact any or all modalities (speaking, understanding, reading or writing) - so it does not follow that because a person is unable to speak they are therefore unable to understand what is being said. Or, just because they can write they can read: a person may for example, have severe difficulties talking but only mild difficulties writing and understanding, as well as a moderate difficulty reading. In this case it may be helpful for this person to have a pen and paper handy to write words down that they aren’t able to say. On the other hand, they could have moderate difficulty understanding another person’s spoken language but have no difficulties reading or in recognising the emotional content of speech; in this instance it would be helpful then for their conversation partner to write words down as they are talking, to slow down and to increase their non-verbal communication.
A person may also present with speech difficulties (rather than, or as well as, a language impairment). So, a person’s facial muscles may not be working as well as they should be causing speech to be slurred/jerky/quiet. If a person has a motor speech impairment such as this, we would not necessarily expect them to have any impairment of comprehension (as it is the muscles that are the problem, not the language) but we may need to help them find a strategy to make themselves understood (using a pen and paper for instance, or using closed questions requiring a yes/no response).
Because of the nature of brain damage, it is rare for one exact and isolated area to be affected but for all other areas to remain unaffected. Often the symptoms caused by stroke or other brain damage do not fit into one neat box. In addition to some of the specific language and communication deficits outlined above, a person may have comorbid difficulties in other areas such as a limb apraxia which causes difficulty with muscle co-ordination; they therefore may have difficulty using gesture to express themselves or using a pen to write. They may have difficulty with executive function, such as short term memory, and so forget what they are saying or what they have just heard, making conversation very challenging. They may have an impairment of planning and monitoring, resulting in their speech going off on tangents and them ‘never getting to the point’, frontal brain damage may result in the production of very inappropriate or disinhibited speech such including swearing or hypersexual language.
No comments:
Post a Comment